“‘It’s going to bankrupt health care’: Spending on temp agency nurses up more than 550% since pre-pandemic at one Toronto hospital network,” ran the headline in the Toronto Star.
“Ontario isn’t ruling out privatization in health care,” was a headline on CBC News.
Temp Agency Nursing is Privatization
Given the shortage of 15,000 nurses since the pandemic began, hospitals across the country have increasingly turned toward agency nurses. However, this stopgap solution is a dangerous symptom of deeper dysfunction in hospitals, existing prior to COVID, where exhausted and underpaid nurses are leaving permanent jobs for flexible gigs at privately owned temp agencies — where they can sometimes earn double their old hourly rate.
“Agency nursing is a form of privatization,” correctly pointed out Doris Grinspun, leader of the Registered Nurses’ Association. In its last fiscal year ending March 2022, the University Health Network (UHN), Canada’s largest research and teaching hospital network, has already spent $6.7 million on agency nurses — up 550 percent from 2018, when it spent $1.035 million. For $6.7m, a hospital could hire 86 nurses and pay them directly instead of being ripped off by for-profit third-party agencies.
The CEO of UHN said, “We’re just not funded to absorb that kind of increase in cost for agency nurses. At the moment, we’re running a deficit to absorb it.” If this continued, UHN would need every year to have an “additional five or six million dollars in order to be in a balanced position.” This is plain outsourcing — finding another $6 million means public money, originally aimed at one part of the health system, being transferred to for-profit agencies.
According to hospital invoices seen by the Toronto Star, one agency was charging hospitals $105 per hour plus HST this summer — nearly double what it was charging last fall. Another agency was charging $110 per hour for temp nurses. Job postings by the same agency advertise hourly wages of $40-$65 per hour for registered nurses and $70-$87 per hour for critical care nurses.
Nurses Pushed into Agencies’ Arms
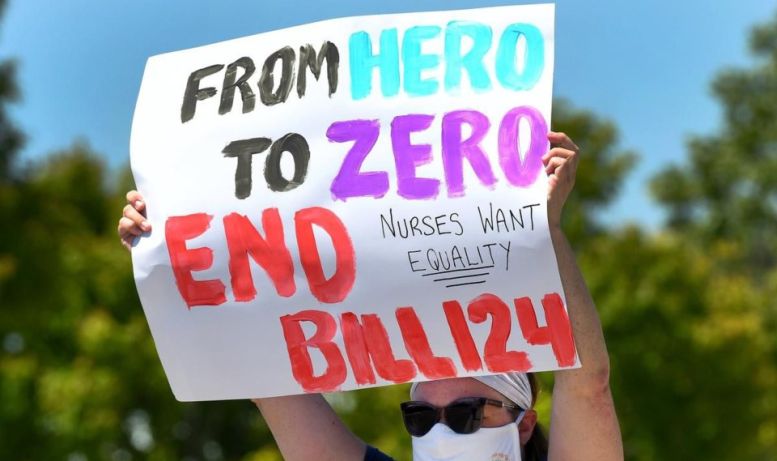
The Ford government’s idea of addressing nurse retention was to offer a one off, lump sum $5000 payment, which the Ontario Nurses Association (ONA) stated was nowhere near what Ford originally informed the ONA it would do. The ONA made clear that this measure is insufficient to address the issues driving nurses away, “which harm patient, resident and client care.” Ford still refuses to repeal the anti-worker wage-suppression law, Bill 124. Enacted in 2019, this attacked all public sector workers, holding down wage increases to one per cent a year. It was yet another piece of Orwellian terminology called the Protecting a Sustainable Public Sector for Future Generations Act.
Apart from bankrupting health care, the growing use of agency nurses has other negative impacts. Agency nurses sometimes do not know patients well, jeopardizing continuity of care and when nurses are unfamiliar with their environment, they may be at greater risk of injury or violence.
Nonetheless, a morale-crushing combination of factors — from stagnant wages and pandemic burnout to soaring living costs — has pushed some nurses into agencies’ arms. Anna Seto, a hospital nurse, was interviewed by the Toronto Star. Sherelated how she quit her nursing job at UHN and joined an agency. Since then, she’s noticed a “drastic improvement” in her well-being and mental health. She was one of the first health workers in Ontario to get COVID on the job during a hospital outbreak in April 2020 and spent most of the pandemic working one of its most demanding jobs: nursing in the ICU. “By April 2022, Seto was feeling overworked, deeply burnt out and disrespected. Health-care workers were facing backlash from the public, she struggled to get time off and the government’s refusal to repeal Bill 124 felt like a slap in the face.”
Seto also said that at times nearly half of the nurses in her ICU were from agencies — and getting paid twice as much. Meanwhile, the agency nurses sometimes added to the workload of staff nurses, who had to show them the ropes or help them access medication storage rooms that require a staff ID.
Getting “Creative”
The shortage of health workers in Ontario hospitals has caused increased wait times, forcing some hospitals to cancel surgeries or even temporarily close emergency departments.
Ford told reporters he’s a strong believer in public health care, but his government is going to “get creative” when looking at how it could be delivered. He said that “everything is on the table” when asked if Ontario is considering further privatization of the health-care system. “There’s one thing we’ll guarantee: you’ll always be covered by OHIP, not the credit card.”
“Are we gonna get creative? Absolutely. As I mentioned, we just can’t as a province keep doing the same thing and expecting a different result.” Earlier this week, Health Minister Sylvia Jones said the government is looking at all options to improve the health system, sparking fears of further privatization. She later said what is not under consideration is asking people to pay out of pocket for services currently covered by the Ontario Health Insurance Plan.
However, the use of nurses from private agencies and sending patients to private health providers increases the costs to the health system, as these companies exist to make profits. It drains staff and services from the public system and often provides poorer quality services and outcomes.
More Beds, Better Care?
It’s not just in the field of subsidizing private health care agencies that Ford is willing to help out the private health sector. The for-profit care homes became death traps during COVID. “Homes with for-profit status had outbreaks with nearly twice as many residents infected … and 78 per cent more resident deaths,” according to Ontario’s science table advising on COVID. Despite this terrible level of deaths, Ford is going to boost their business. As Socialist Alternative wrote, “Doug Ford would have us believe that the deaths of 249 people (April 20, 2020) in residential care homes are just an unfortunate aspect of the COVID-19 crisis. In reality, it’s a case of a chronicle of deaths foretold.” Yet, Ford still wants to help the for-profit owners out by making an already flawed system worse. Justified by the claim to free up acute care beds in hospital, Bill 7 will allow the forced transfer of patients from hospitals to LTC homes if they are deemed not to require acute care.
Ford has rushed through (without any parliamentary committees or public hearings) legislation known by its Orwellian title More Beds, Better Care Act. The decision to move to long-term care — or the decision to move a family member there — is a major life decision. Like any move, it’s one that has profound consequences not just for where a person lives but how they live. It’s no surprise that many resist the move, especially given the bad reputation acquired by many of these homes during the pandemic.
Currently, those seeking long-term care have some choice in the matter. This may allow them to live in a nursing home close to family members. Ford’s reforms would remove all choice. Officials would be able to dictate where nursing home residents receiving care are able to live. Both the NDP and Liberals have alleged that the regulations supporting the legislation would allow for patients in northern Ontario to be moved up to 300 km from their homes. There is also the question of financial penalties if a hospital patient refuses to be moved to a LTC home Young or old, staying in hospital if once a person is cleared for discharge to available care elsewhere, could cost $400 a day as the Ontario government tries to free up beds for the expected fall and winter surge of COVID-19 and flu.
The pandemic has been particularly hard on older people living in long-term care. In part, that has been the result of families being banned from homes where they could help care for their senior relatives. Ford’s reforms favour for-profit nursing homes and penalize those residents searching for spaces close to home.
Profiting from Health, a Slippery Slope
Harold Macmillan, former British Tory Prime Minister from the 1950s, criticized Margaret Thatcher’s program of privatization. “First of all the Georgian silver goes, and then all that nice furniture that used to be in the saloon. Then the Canalettos go.” Of course, Thatcher’s privatizations were on a much grander scale (water, steel, British Airways, and telecoms, among others) than that being contemplated, so far, in Ontario. But Thatcher did also privatize care homes. And Macmillan’s point is valid. You start with one privatization and then you’re on a slippery slope. It is said that appetite comes with the eating. It doesn’t come much bigger than the appetite of big business for profits, especially when they get handed to them on a plate.
Already large parts of Canada’s health system are run for profit — many care homes, dentists and opticians, pharmaceuticals and most family doctors are separate businesses. This drive for ever more profits is a constant threat to providing public health. As Ontario’s seniors’ homes clearly demonstrate, who provides services — the publicly owned or the for-profit sector — makes a real difference.
Health unions, the public and the NDP need to build a mass movement to resist Ford’s latest moves to help the profit seekers from leaching off the public purse.
Longer-term, Canada needs a fully public health system with all parts of health care under democratic control. And health care needs to be expanded to preventative measures and to tackling the deep inequalities of society that are the key social determinants of public health.


